We can help prevent hospital-acquired infections during renovation
January 10, 2018
January 10, 2018
Controlling dust and air pressure—and future-proofing buildings for renovation—can save lives
Ideally, hospitals return patients to home in better condition than when they entered. But the hospital environment itself can pose risks to patient well-being. Hospital-acquired infections (HAI) are the third highest leading cause of death in the United States. The Centers for Disease Control and Prevention estimate that 1.7 million HAIs occur in US hospitals every year, resulting in almost 100,000 deaths. Some of these deaths are directly related to design and construction.
A significant percentage of HAIs are a result of construction dust generated during renovation projects.
How does this happen? Construction brings more bodies, materials, dust, harsh chemicals, and accompanying bacteria into the healthcare environment. This traffic of people and things allows particulates and bacteria to travel deeper into the facility. Add vibration and noise of construction into the mix and you’ve got more dust and mold spores blowing around as well as disruption to patients and sensitive instruments. Demolition, for example, can release bacteria and mold into the facility.

The North Island Hospital Comox Valley, a 153-bed facility in Courtenay, British Columbia.
Practices for infection control during renovation exist but they are still evolving and some current practices may be inadequate. For example, required infection control during renovation measures are typically reactive to the risk at hand, rather then integrated into the facility. Because hospitals are dynamic, healthcare designers are accustomed to designing for future flexibility. But we don’t necessarily plan for infection-control measures required for an inevitable renovation.
One of the first steps in any healthcare renovation project is to set up systems to control the migration of dust particles between the construction area and other occupied areas of the healthcare facility. It’s a generally accepted infection-control practice—and in some regions even mandated by codes and standards—that contractors use portable negative air HEPA filtration units to control dust, relative air pressures, and airflow direction during renovations. Portable exhaust fans and filters draw thousands of cubic feet of air per minute from the construction zone, filter some 99.9% of airborne contaminates from that air, and then discharge the air to the outside of the building.
A consistent challenge with this type of setup, however, is figuring out how to create a temporary path for these exhaust fans to get their dirty air out of the building. The solutions I commonly see are rarely elegant. To use these negative air units, contractors must drag large-diameter flexible ducts down hallways. Sometimes, I see them propping open fire doors and swapping windows for plywood and duct-tape contraptions.
But progress is possible. We’d do better to welcome a recent evolution in healthcare building design which anticipates and accommodates the future use of these negative air units during renovations or expansions.
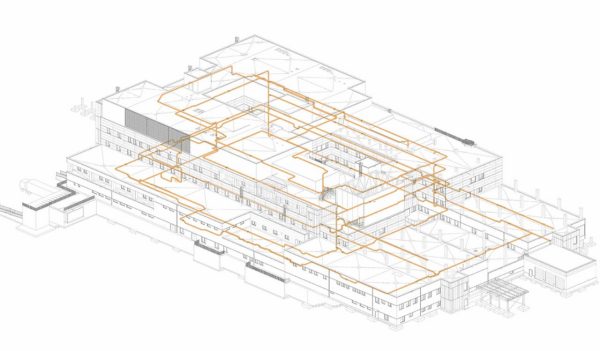
A Revit model for the recently completed North Island Hospital Comox Valley shows the implementation of a permanent negative air duct running throughout the building.
Thankfully, we’re seeing significant progress in building design solutions to this issue. Cutting-edge hospitals are now installing dedicated negative air ducting systems designed to provide a pathway for the safe removal of this dirty air from future renovation sites. On a recent replacement hospital project, the system consisted of “loops” of 350mm round spiral ducts installed in the ceiling spaces within each department of the hospital. The duct loops all combine in a central mechanical room, where a dedicated exhaust fan helps discharge the dirty air to the outside of the building.
Now when renovation projects occur, the contractors simply need to locate the nearest negative air duct, create whatever number of quick connections are required to each so they can hook up a portable negative air unit. The main fan in the mechanical room ensures that the entire loop is under negative air pressure and the local portable fans take care of the filtration and getting the air into the loop.
These pre-planned connection points in interior areas of the hospital are especially valuable, as finding routes to the exterior in deep-floor plate hospitals can be extremely challenging.
Anticipating the air exhaust requirements of future renovation projects can also help us to reduce construction costs, mitigate the fire hazard risk associated with temporary duct routings, and decrease the chance that negative air systems are incorrectly configured during construction. Ultimately, if these practices help reduce the occurrence rate of hospital-acquired infections in our facilities, they’re worth the time and effort.
